What is Double Outlet Right Ventricle?
Double outlet right ventricle (DORV) is a congenital heart defect and is characterized by the two major arteries of the heart, the pulmonary artery and the aorta, both connecting to the right ventricle of the heart 1–3. Typically, the aorta is connected to the left ventricle of the heart and pumps oxygenated blood around the body, while the pulmonary artery is connected to the right ventricle and takes deoxygenated blood to the lungs. In DORV, since both arteries connect to the right ventricle, the aorta pumps deoxygenated blood around the body instead of solely oxygenated blood. Patients with DORV are also born with a ventricular septal defect, which is a hole in the wall between the lower heart chambers (the right and left ventricles). Thus, in DORV, deoxygenated blood enters the right atrium, flows into the right ventricle and is pumped to the lungs to become re-oxygenated. However, simultaneously, oxygen-poor blood is also pumped out through the aorta to the rest of the body. The ventricular septal defect means that any re-oxygenated blood from the lungs that enters the left atrium and ventricle is able to mix with the oxygen-poor blood, but even with this oxygen-rich blood mixing in with the oxygen-poor, there is still not enough oxygen being delivered to the rest of the body and the heart has to work harder. This can also mean that the lungs receive more blood volume than usual, and this can be problematic.3 However, without the ventricular septal defect, the newly oxygenated blood from the lungs would have no place to go, so initially it helps to keep the newborn alive.
DORV is classified into different subtypes based on the location of the ventricular septal defect and the arrangement of the major arteries. In addition, there may be problems with the heart valves, other blood vessels, or other holes in the heart. In some cases, patients may also have pulmonary stenosis, a condition whereby the valve connecting the right ventricle (the heart) to the pulmonary artery (leading to the lungs) is not able to open or function properly. Additionally, there may be abnormalities in the mitral valve, which separates the left atrium from the left ventricle.1,3
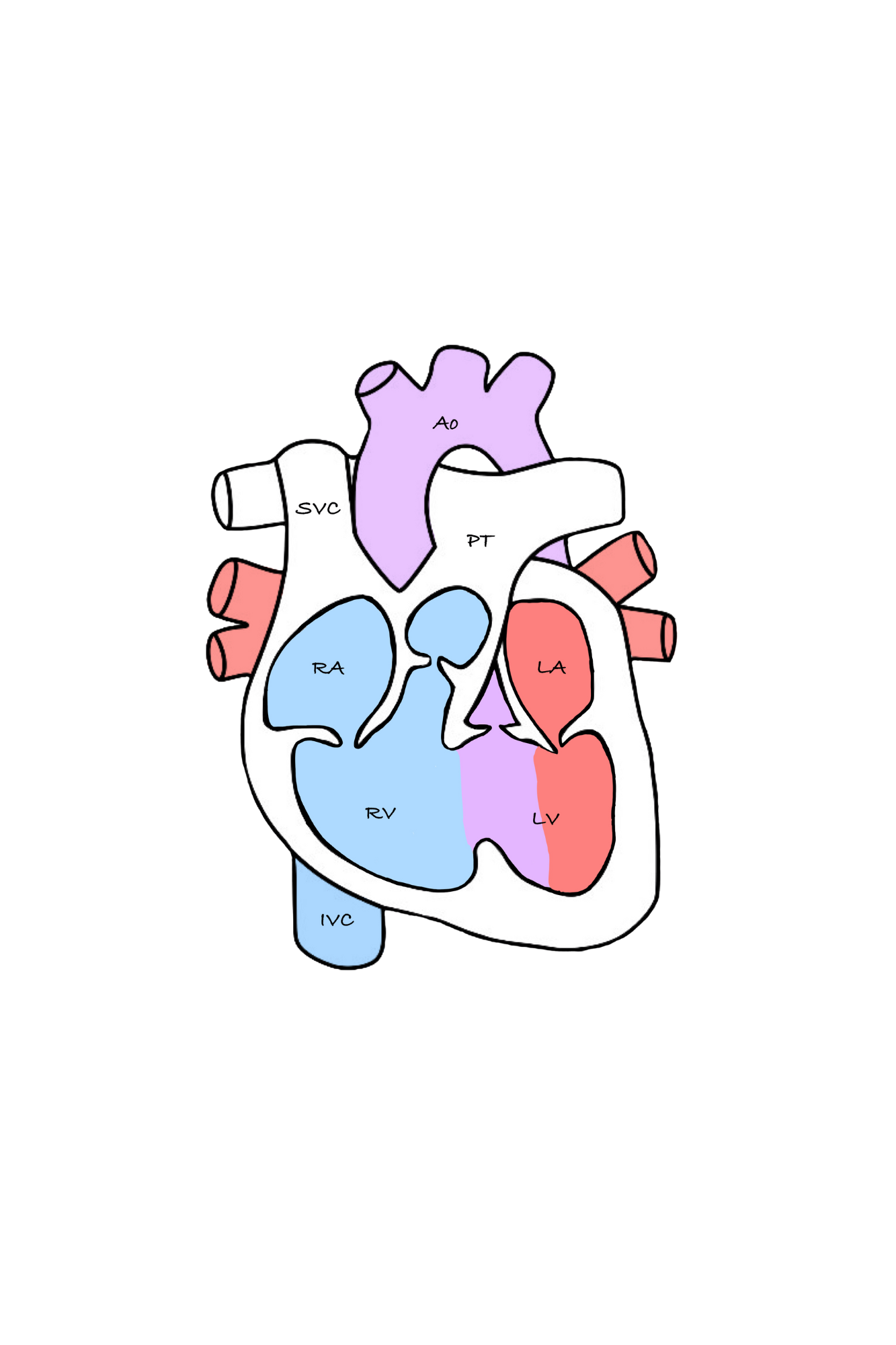
Double outlet: Pulmonary artery and aorta both connect to the right ventricle.
Ventricular septal defect: re-oxygenated blood from the lungs that enters the left atrium and ventricle is able to mix with the oxygen-poor blood
Symptoms: 2,3
Sweating, especially with feeding
Unresponsiveness
Rapid heartbeat
Heart murmur, an abnormal heart sound when the doctor checks with a stethoscope
Failure to thrive or gain weight
Blue or purple coloring of lips, skin, nail bed (referred to as cyanosis)
Shortness of breath or rapid breathing
Difficulties in feeding
Fatigue or more sleepiness than normal
DORV can be diagnosed during pregnancy or postnatally.2,3 Prenatal ultrasound may detect some congenital heart defects, and if so, this is followed up by a cardiac ultrasound. However, if it is not diagnosed during pregnancy then after the child is born, DORV is often diagnosed by means of:1–4
Diagnosis

Echocardiogram (Echo)
Note: A cardiac CT is the preferred diagnostic and surgical planning tool for DORV because of its high level of accuracy in displaying the various structures within or entering into the heart.
Cardiac MRI/CT
Chest X-ray (CXR)

Electrocardiogram (EKG)

Pulse Oximetry

Cardiac Catheterization
Treatments
Some babies with DORV need heart repair surgery within the first few days of birth, while other patients may have surgery within a few months of birth.1 There are several types of surgery that can be done that are entirely dependent on the specific subcategory of DORV. Among the various surgical options, the most common procedure for addressing DORV with a ventricular septal defect (VSD) is intraventricular tunnel repair. In this procedure, the surgeon constructs a tunnel to link the left ventricle to the aorta and places a patch to guide blood flow from the left ventricle to the aorta.2
Surgery may involve one or more of the following:
Connect the LV to the aorta via a tunnel the surgeon creates or the surgeon may need to correct the positions of the aorta and pulmonary artery if their positions are reversed. This would involve connecting the pulmonary artery to the right ventricle and the aorta to the left ventricle.
Close the opening between the lower chambers of the heart to stop blood mixing once the vessels are correctly positioned and connected.
If the pulmonary artery is small and narrow, the surgeon may either expand the pulmonary artery or insert an additional blood vessel from the right ventricle to the pulmonary artery to increase blood flow.
In certain newborns, a temporary shunt may be put in place to increase blood flow to the lungs. The surgeon will place a shunt between the baby’s aorta and pulmonary artery (often referred to as a patent ductus arteriosus). This shunt is typically removed after the other surgeries to repair DORV.
Additional Resources
References
Mayo Clinic Staff. Congenital heart defects in children. Mayo Clinic. December 7, 2024. Accessed January 12, 2025. https://www.mayoclinic.org/diseases-conditions/double-outlet-right-ventricle/cdc-20389537
Boston Children’s Hospital. Double Outlet Right Ventricle (DORV). Boston Children’s Hospital. Accessed January 12, 2025. https://www.childrenshospital.org/conditions/dorv
Children’s Hospital of Philadelphia. Double Outlet Right Ventricle. Children’s Hospital of Philadelphia. https://www.chop.edu/conditions-diseases/double-outlet-right-ventricle
Hyun Woo Goo. Double Outlet Right Ventricle: In-Depth Anatomic Review Using Three-Dimensional Cardiac CT Data. National Library of Medicine. September 13, 2021. Accessed January 12, 2025. https://pubmed.ncbi.nlm.nih.gov/34564964/